Date Added : 1989-10-01
2.1.0.1 Definition
Date of emergence from Post-traumatic Amnesia (PTA).
Where possible, PTA emergence should be measured (tracked) prospectively by direct testing. With prospective tracking, emergence from PTA is defined as:
- two consecutive GOAT scores of 76 or greater with no more than 2 full calendar days between assessments (Assessment 1 = Friday, Assessment 2 = Monday, two full days = Saturday, Sunday)
- two consecutive scores of 11 or greater on the Revised GOAT with no more than 2 full calendar days between assessments (Assessment 1 = Friday, Assessment 2 = Monday, two full days = Saturday, Sunday)
- two consecutive scores of 25 or greater on the Orientation-Log with no more than 2 full calendar days between assessments (Assessment 1 = Friday, Assessment 2 = Monday, two full days = Saturday, Sunday)
- two consecutive scores of 8 or greater on the Non-Verbal version of the Orientation-Log with no more than 2 full calendar days between assessments (Assessment 1 = Friday, Assessment 2 = Monday, two full days = Saturday, Sunday), or
- in the judgment of a qualified clinician (i.e., speech-language pathologist, physician, neuropsychologist), the person has cleared PTA but administration of an orientation test is not possible due to language functioning.
The day of clearance of PTA is the first day the person gets the first of 2 consecutive scores of 76 or greater on the GOAT, the first of 2 consecutive scores of 11 or greater on the Revised GOAT, the first of 2 consecutive scores of 25 or greater on the Orientation-Log, or the first of 2 consecutive scores of 8 or greater on the Non-Verbal version of the Orientation-Log.
If within a 7-day period, there are multiple scores exceeding the PTA cut-off, but the first two are separated by more than two full calendar days (e.g. Assessment 1 = Friday, Assessment 2 = Tuesday; this would be 3 full calendar days apart), then it is acceptable to use the midpoint between the first and second dates the PTA assessment was administered.
It is the choice of the Project Director as to whether to use the GOAT, Revised GOAT (Bode, Heinemann, & Semik, 2000 – see SOURCES) or the Orientation-Log (Jackson, Novack, & Dowler, 1998; Novack, Dowler, Bush, Glen, & Schneider, 2000 – see SOURCES) to establish the duration of PTA. Alternating use of the scales in an individual patient is not acceptable, however. Preferably, copies of the test protocols documenting PTA tracking should be kept in the research record. If the PTA data is elsewhere (e.g., in the rehabilitation chart), the location should be noted in the research record.
The Non-Verbal version of the Orientation-Log is the preferred assessment of orientation for persons with traumatically induced expressive language disorder with significant difficulty generating comprehensible verbal output. Common causes for this problem include expressive aphasia and severe dysarthria accompanied by an inability to write responses. Non-verbal responses are scored according to the following criteria: 1 = correct upon multiple choice / 0 = incorrect or no response. This scoring adjustment is intended to be used only for non-verbal individuals with significant difficulty generating comprehensible verbal or written output. Careful clinical judgment will be required in each case to determine that the person’s expressive problems are clearly due to neurological disorder, and the person is unable to respond in writing.
Determining Date of PTA Emergence During Acute Care
For those patients who are already oriented at rehabilitation admission (as defined by the first two GOAT scores after rehabilitation admission >75), prospective tracking of the date of emergence from PTA is not possible, because the date falls within the acute care stay. In these cases, PTA emergence can be determined via chart review of the acute care records only. (NOTE: Rehabilitation hospital charts may NOT be used for this purpose). The following procedure can be used to determine the length of PTA based on acute care hospital records. This procedure should be followed only for those patients who are oriented at rehabilitation admission.
Obtain all available physician, nursing and therapy notes from the acute hospitalization. In most hospital medical records, physician, nursing and therapy notes are filed in different sections. You may have to specifically request therapy and nursing notes, if you routinely only receive the physician progress notes.
Review all notes to determine the first DATE on which all notes referencing orientation indicate that the patient is fully oriented, oriented X 3 (or 4), or GCS Verbal Score = 5 (oriented). This is Orientation Day 1.
Review notes from the next calendar day to determine if all relevant notes again indicate that the patient is fully oriented.
If yes, the second day is Orientation Day 2, and Orientation Day 1 is the resolution date of PTA. If there are missing notes or no comments about orientation on the second day, keep looking for the second day that the notes consistently document full orientation. As long as Orientation Day 2 is no more than 2 full calendar days from Orientation Day 1, and if no notes from intervening days indicate less than full orientation, record Orientation Day 1 as the resolution date of PTA.
If any note from calendar days intervening between Orientation Days 1 and 2 indicate less than full orientation, use Day 2 as the new starting point (i.e., new Day 1) and repeat procedure from Step 3 above.
If there is no Orientation Day 2 (i.e., if the patient is never fully oriented on more than one day; or if more than 2 full calendar days elapse after Orientation Day 1 with no further notation about orientation), code date of PTA resolution as unknown. An exception would be if on the day before or the day of transfer to rehabilitation, the patient is specifically noted not to be oriented. If the patient then produces GOATs >75 on the first two examinations after rehabilitation admission, code the date of PTA resolution in the usual manner.
2.1.0.2 Form
[X] Form 1
[ ] Form 2
2.1.0.3 Source
Form 1 - Abstraction (acute record only) or measured by direct O-Log or GOAT testing (rehab record)
2.1.0.4 Details
Administer the test every 1 to 3 calendar days until patient emerges from PTA.
There is no code for “unknown” for method of PTA determination because this should never be unknowable. Please contact the TBINDC if you are in a situation in which this variable is truly unknown (and unknowable).
Code date of admission to ER if person was never in PTA.
If PTA lasts less than 24 hours, code day 2 as the date of emergence from PTA, since this would be the first day that they were fully oriented.
If participant was not out of PTA at Rehab discharge score is coded as “888. Person Still in PTA at time of Rehab Discharge”.
If a person was never in PTA the days = 0.
For cases who do not emerge from PTA by rehab discharge, code the method used to decide if the patient is still in PTA.
The same instrument must be used for all scores to capture the date emerged from PTA during rehabilitation. GOAT and O-Log scores may not be mixed and matched.
Record review can not be used to determine Date Emerged from PTA during rehab. If PTA was not tracked with GOAT or O-Log during rehab and patient did not emerge during the acute stay, Date Emerged from PTA should be coded as “09/09/9999 (Unknown)”, and Method of Determination should be coded as “88. (N/A PTA Not Tracked)”.
Patients who don’t have any documented GOAT or O-Log scores possibly due to other cognitive deficits (e.g. “confused due to dementia’‘) and formal testing may not have been possible should be’‘09/09/999 - Unknown’’ rather than ‘’08/08/8888 - Never Emerged.’’ The method of PTA determination should be coded as ‘88. PTA has not been tracked.’. Record review cannot be used to determine emergence from PTA during rehab.
If an acute record states “patient is A&O x3 with choices”, and the patient has aphasia or some other expressive language disorder, then testing with choices would be appropriate to asses orientation and would count as being oriented.
Computer calculates duration of post-traumatic amnesia by subtracting the date of injury from this date.
Duration of PTA is calculated only for those cases which emerge from PTA prior to discharge from inpatient rehabilitation.
Duration of PTA is not to be calculated from date of emergence from coma [FLLW], per decision of the neuropsychology databusters group.
Two consecutive GCS Verbal scores of “5-Oriented” may be used to determine length of PTA when there is no other source of documentation using acute chart review.
For cases who never had PTA, code “Method of PTA Determination” as “1-Acute Chart Review”.
2.1.0.5 Links
PTA - Introduction to O-Log (COMBI)
PTA - O-Log frequently asked questions (COMBI)
PTA - O-Log Syllabus (COMBI)
PTA - O-Log Rating Form (COMBI
PTA - O-Log Properties (COMBI)
PTA - O-Log References (COMBI)
PTA - Bode RK, Heinemann, AW, Semik P. for v144a
PTA - Jackson WT, Novack TA, Dowler RN for v144a
PTA - Novack TA, Dowler RN, Bush BA, Glen T, Schneider JJ. for v144a
PTA - Levin, HS, O’Donnell, VM, & Grossman, RG for v144a
2.1.0.6 Reference
GOAT: Levin, HS, O’Donnell, VM, & Grossman, RG. (1979). The Galveston Orientation and Amnesia Test: A practical scale to assess cognition after head injury. Journal of Nervous and Mental Diseases, 167, 675-684. See External Links
Revised GOAT: Bode RK, Heinemann AW, Semik P. Measurement properties of the Galveston Orientation and Amnesia Test (GOAT) and improvement patterns during inpatient rehabilitation. J Head Trauma Rehabil. 2000 Feb;15(1):637-55. See External Links
Orientation-Log (and Non-Verbal version of the Orientation-Log): Jackson WT, Novack TA, Dowler RN. Effective serial measurement of cognitive orientation in rehabilitation: the Orientation Log. Arch Phys Med Rehabil. 1998 Jun;79(6):718-20. Link to PubMed: See External Links
Novack, TA, Dowler, RN, Bush, BA, Glen, T, Schneider, JJ. Validity of the Orientation Log, Relative to the Galveston Orientation and Amnesia Test. J Head Trauma Rehabil, 2000, 15(3), 957-961. See External Links
2.1.0.7 Characteristics
A few participants have a very long time in PTA. These have been checked and found to be correct.
A modified GOAT can be used to assist with this decision. The examiner presents three alternatives, in written form and orally, including the correct choice for each question. The patient is to indicate a choice in some manner, such as nodding or pointing. This procedure can be used for all questions except numbers 4 and 5. The three response alternatives for each question should be arranged vertically in large print on an index card. Error points are assigned and subtracted from 80 (the maximum score with items 4 and 5 removed). A score of 61 or higher is reflective of orientation. PTA is considered resolved when a score of 61 or greater is achieved on two consecutive occasions with no more than 2 full calendar days between assessments (Assessment 1 = Friday, Assessment 2 = Monday, two full days = Saturday, Sunday). Scores from the modified GOAT are for determination of PTA duration only.
There are 3880 in PTA at the time of discharge.
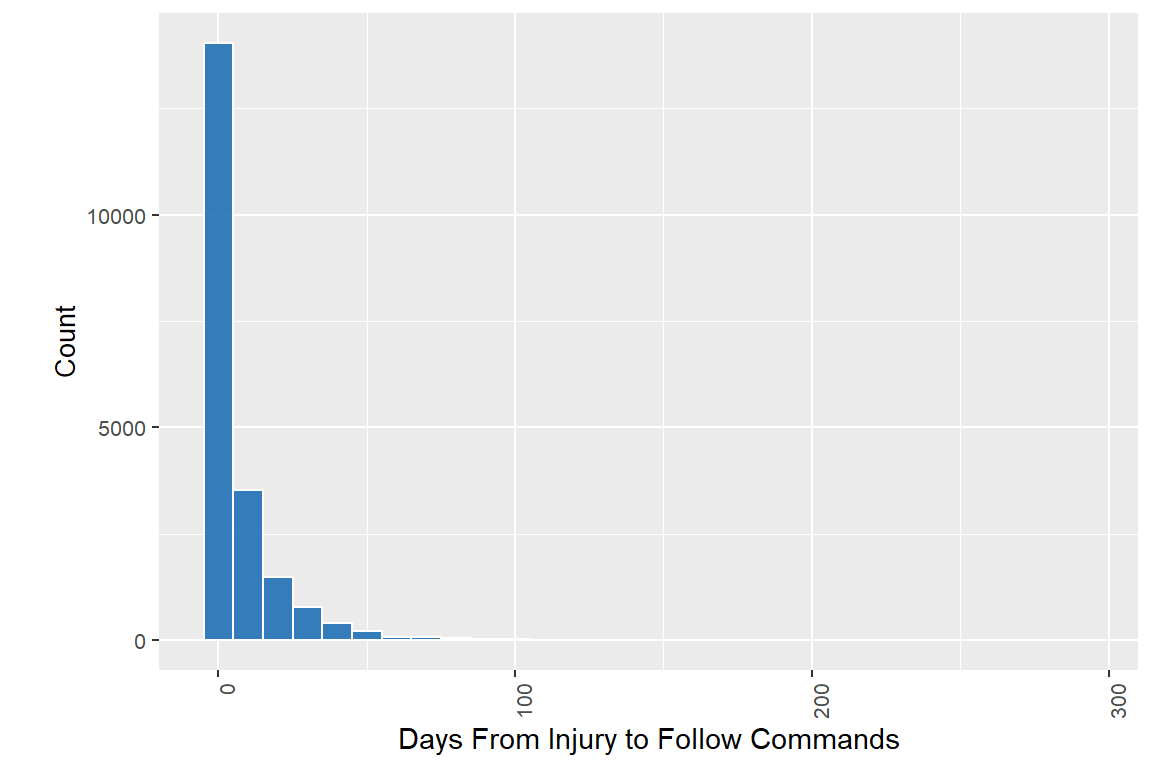
| Days From Injury to Date Out of PTA | |
| Characteristic | N = 21,526 |
|---|---|
| Days From Injury to Date Out of PTA | |
| N Non-missing | 16,789 |
| Mean (SD) | 22 (22) |
| Median (Q1, Q3) | 17 (5, 32) |
| Min, Max | 0, 361 |
| Unknown | 4,737 |
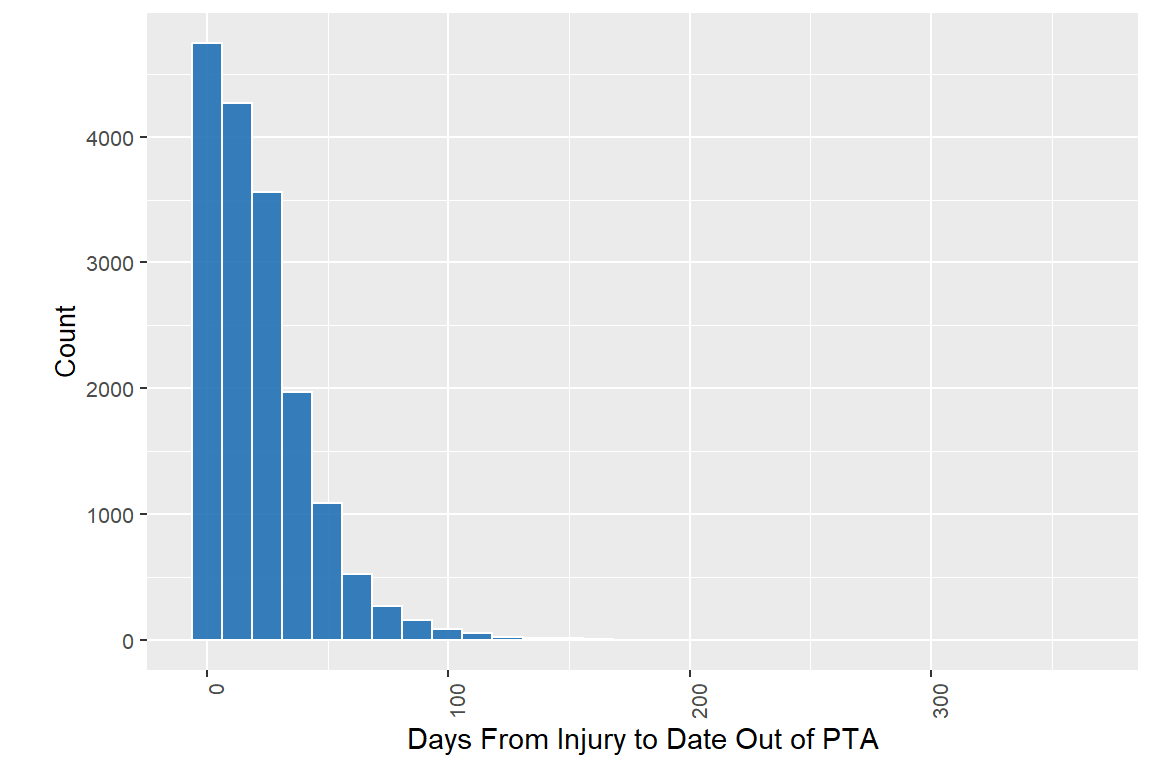
78% of the abstracted people have valid data