Caution
FIM Motor was replaced by the Continuity Assessment Record and Evaluation on 7/1/2020. Therfore FIM Motor and Total Score data will not be represented after that date for Admission and Discharge. However it is still collected at Follow-up
FIM Motor was replaced by the Continuity Assessment Record and Evaluation on 7/1/2020. Therfore FIM Motor and Total Score data will not be represented after that date for Admission and Discharge. However it is still collected at Follow-up
Date Added : 1989-10-01
The FIM instrument is a measure of disability. It is intended to measure what the person with the disability actually does, not what he or she ought to be able to do, or might be able to do if certain circumstances were different. It is to be completed based on assessment over 3 calendar days for each assessment period.
FIM instrument data are to be collected according to the current (10/01/2012) IRF-PAI coding instructions (see External Links, supplemented by any further instructions in your syllabus). Information about the FIM instrument can be found in the IRF-PAI manual in section III, pages 39-95. If it is not possible for your Center to follow the correct manual, notify the TBINDC.
At Form 1, only Cognitive FIM items are collected.
The rating scale below should be used for each item. The syllabus provides additional detail on the ratings specific to the items.
Ratings should be based on the poorest performance during the 72-hour assessment period.
Rating Scale
7 - Complete Independence (Timely, safely)
6 - Modified Independence (Extra time, device)
5 - Supervision (performs 100%, but needs supervision)
4 - Minimal Assist (>= 75%)
3 - Moderate Assist (50 - 74%)
2 - Maximal Assist (25 - 49%)
1 - Total Assist (< 25%)
[X] Form 1
[X] Form 2
Form 1 - Abstract from FIM form (rehab record)
Form 2 - Interview (participant or proxy)
All FIM items have an “assessment time period”. The assessment time period for all FIM items (except Bladder and Bowel Frequency of Accidents) is 3 days.
Scoring reflects the patient’s poorest (most dependent) functioning during the assessment time period. The evaluation is therefore not a snapshot of the patient’s performance at the time of evaluation, but a summary of performance over the entire assessment time period.
All FIM items must be scored. Record what patient actually does. If FIM assessment cannot be completed within the window of 3 calendar days, it should still reflect the patients’ status within that time period. If this is not possible and the assessments are done out of the window of 3 calendar days, code as “Unknown”. Every effort should be made to obtain the FIM assessments; however, if any items are not assessed, code “Unknown.” Do not leave blanks.
According to the UDS Procedures for Scoring the FIM instrument, “if the subject would be put at risk for injury if tested or does not perform the activity, enter 1.” Use this same rule for the TBI Model Systems FIM instrument data collection.
For Eating, Grooming, Bathing, Dressing Upper and Lower Body, Toileting and Transfers, if activity is not performed, assign code “1. Total Assist” (do not use the “0” code at follow-up).
The “Unknown” code is specific to the Model Systems and is to be used when the activity was not assessed within the window due to site specific reasons (e.g. therapists were unable to track patient down to assess FIM item.) At discharge, if an item is not assessed because the patient does not perform the activity, (e.g., patient is unable to perform activity due to an illness or other reasons, or it is unsafe for them to perform the activity) it should be coded as a “1-Total Assistance”. If the patient was being evaluated at admission with either of these reasons, the score would be a “0”.
If patient has an intermittent acute care stay during inpatient rehabilitation, use the FIM scores from the first rehabilitation admission and the last definitive discharge. In addition, if a patient has an intermittent stay which is longer than 30 days, it is then considered a system discharge and the discharge date from rehabilitation is the system discharge date and the FIM scores should correspond to that date.
The patient’s score on measures of function should not reflect arbitrary limitations or circumstances imposed by the facility. For example, a patient who can routinely ambulate more than 150 feet throughout the day with supervision (score of 5 for FIM Locomotion: Walking/Wheelchair item), but who is observed to ambulate only 20 feet at night to use the toilet because that is the distance from his/her bed, should receive a Walk score of 5 rather than a lower score (IRF-PAI Training Manual 1/16/02, page III-4).
FIM scores may be abstracted from the medical record as long as the notes are specific (e.g. “patient feeding themselves independently”; “patient is unable to ambulate”; “patient needs the assistance of two people for all transfers”).
If a patient expires while in the rehabilitation facility, record a score of Level 1 for all discharge FIM items.
Total admission FIM is calculated using the admission walking score if participant is walking at discharge or the admission wheelchair score if the person is in a wheelchair at discharge.
At follow-up, FIM may be asked of anyone who would know the details of the participant’s functioning in these areas.
FIM Manual - IRF-PAI instructions for FIM data collection
Introduction (COMBI)
Summary of the differences between the 4/2004 instructions and the 1/2002 instructions
FIM Decision Rule
FIM Cognitive Rating Form
Fone FIM for TBIMS * Fone FIM to be used only as a supplement to assist as needed in determining FIM scoring - not as word-for-word administration.
Uniform Data System for Medical Rehabilitation 232 Parker Hall SUNY South Campus 3435 Main Street Buffalo, New York 14214 3007 (716) 829 2076; FAX (716) 829 2080
The IRF-PAI instructions for the FIM instrument are disseminated through the website of The Centers for Medicare and Medicaid Services. For information about the CMMS, go to: http://www.cms.hhs.gov/researchers/projects/APR/2003/facts.pdf.
©1997 Uniform Data System for Medical Rehabilitation (UDSMR), a division of UB Foundation Activities, Inc. FIM is a trademark of Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc. This version of the FIM instrument has been modified with permission from UDSMR for use by the Traumatic Brain Injury Model Systems.
12 additional FAM items were collected from 10/01/1989 to 4/01/1998 when the collection of the FAM items became optional. FAM items were removed 7/01/1999.
On 4/1/02 new fields were created to accept data collected with the new (1/1/02) IRF-PAI instructions. The old fields are still in the database. At present there are no calculated variables that merge old data and with new data. Calculated variables based on either old or new scoring are available.
On 10/1/2019, centers began collecting the CARE Item Set at Form 1, and the collection of FIM Motor variables at Form 1 was no longer required. FIM Cognitive variables continue to be collected.
On 7/1/2020, the collection of FIM Motor variables at Form 1 was discontinued.
On 1/15/2025, a new coding rule was implemented: “If all FIM Cognitive items = 7 and FIM Stairs = 7, then remaining FIM items can be skipped and coded as 7.”. FIM Cognitive questions are now asked first, followed by FIM Stairs and the remaining FIM Motor items in the standard FIM order.
Testing and certification of data collectors of this variable is required. Check with your center for their requirements for FIM certification.
ITHealthTrack training and certification materials (DVDs) are available at each local TBIMS center and also on the website under the Training & Certification tab (click on the “Certification” dropdown, then “Certification File Manager”, then “FIM Certification Materials”. Please contact CB Eagye at “PEagye@craighospital.org” for additional training and certification details.
A score of 80% or greater is required for FIM certification.
See external links for ITHealthTrack Exam Instructions and Exam Form.
| FIM Total | |||||||||||
| Characteristic | ADM N = 18,309 |
DIS N = 18,309 |
Year 1 N = 17,114 |
Year 2 N = 15,144 |
Year 5 N = 11,895 |
Year 10 N = 8,062 |
Year 15 N = 4,984 |
Year 20 N = 2,469 |
Year 25 N = 875 |
Year 30 N = 255 |
Year 35 N = 39 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| FIMTOT | |||||||||||
| N Non-missing | 17,431 | 17,530 | 16,085 | 14,168 | 11,158 | 7,483 | 4,575 | 2,254 | 747 | 216 | 29 |
| Mean (SD) | 51 (23) | 90 (23) | 113 (20) | 114 (19) | 115 (18) | 116 (17) | 116 (17) | 117 (16) | 116 (16) | 116 (14) | 117 (14) |
| Median (Q1, Q3) | 51 (30, 69) | 94 (79, 107) | 120 (111, 124) | 121 (113, 125) | 122 (115, 125) | 122 (116, 125) | 122 (116, 125) | 122 (116, 125) | 121 (114, 124) | 120 (112, 124) | 123 (115, 126) |
| Min, Max | 18, 126 | 18, 126 | 18, 126 | 18, 126 | 18, 126 | 18, 126 | 18, 126 | 18, 126 | 18, 126 | 41, 126 | 70, 126 |
| Missing | 878 | 779 | 1,029 | 976 | 737 | 579 | 409 | 215 | 128 | 39 | 10 |
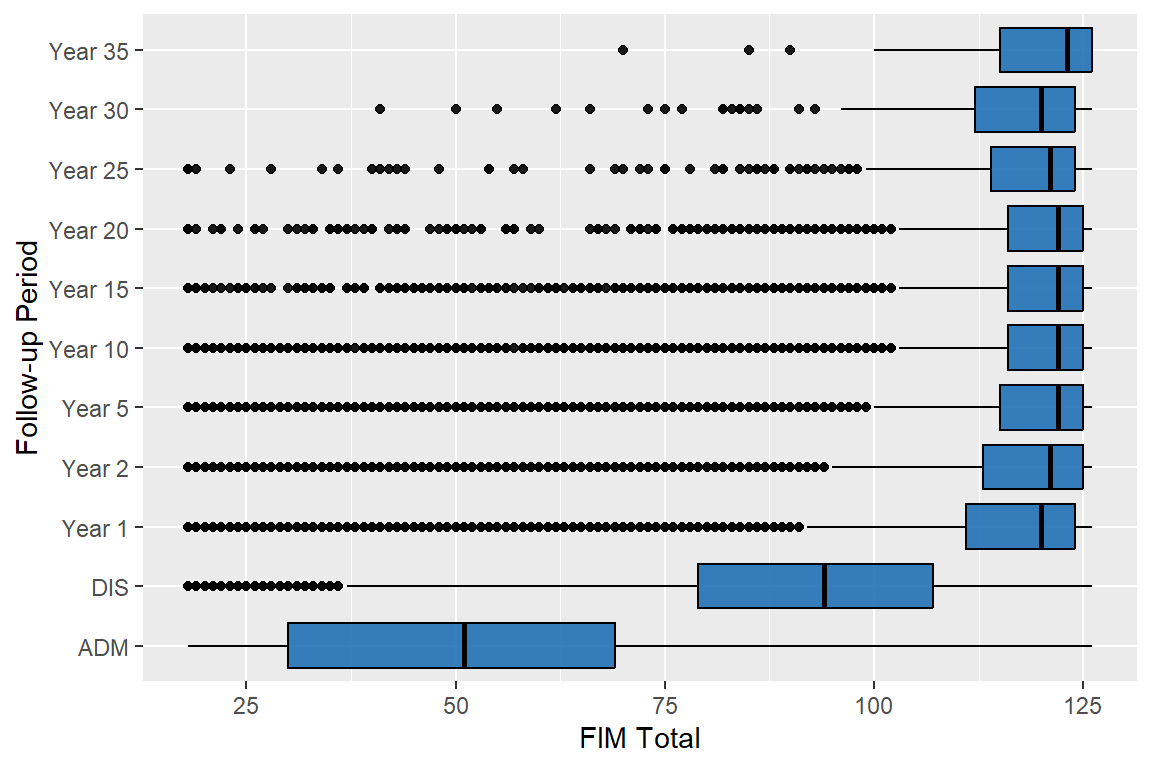
95% of the abstracted people have valid data
93% of the interviewed people have valid data
| FIM Cognitive | |||||||||||
| Characteristic | ADM N = 21,526 |
DIS N = 21,526 |
Year 1 N = 17,114 |
Year 2 N = 15,144 |
Year 5 N = 11,895 |
Year 10 N = 8,062 |
Year 15 N = 4,984 |
Year 20 N = 2,469 |
Year 25 N = 875 |
Year 30 N = 255 |
Year 35 N = 39 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| FIMCOG | |||||||||||
| N Non-missing | 21,025 | 20,952 | 16,253 | 14,288 | 11,244 | 7,538 | 4,598 | 2,265 | 751 | 218 | 29 |
| Mean (SD) | 16 (8) | 24 (7) | 30 (6) | 31 (5) | 31 (5) | 31 (5) | 31 (5) | 31 (4) | 31 (5) | 31 (5) | 32 (4) |
| Median (Q1, Q3) | 15 (9, 22) | 25 (20, 29) | 32 (29, 34) | 32 (29, 34) | 33 (30, 34) | 33 (30, 34) | 33 (30, 34) | 33 (30, 34) | 33 (30, 34) | 32 (30, 34) | 34 (30, 35) |
| Min, Max | 5, 35 | 5, 35 | 5, 35 | 5, 35 | 5, 35 | 5, 35 | 5, 35 | 5, 35 | 5, 35 | 8, 35 | 21, 35 |
| Missing | 501 | 574 | 861 | 856 | 651 | 524 | 386 | 204 | 124 | 37 | 10 |
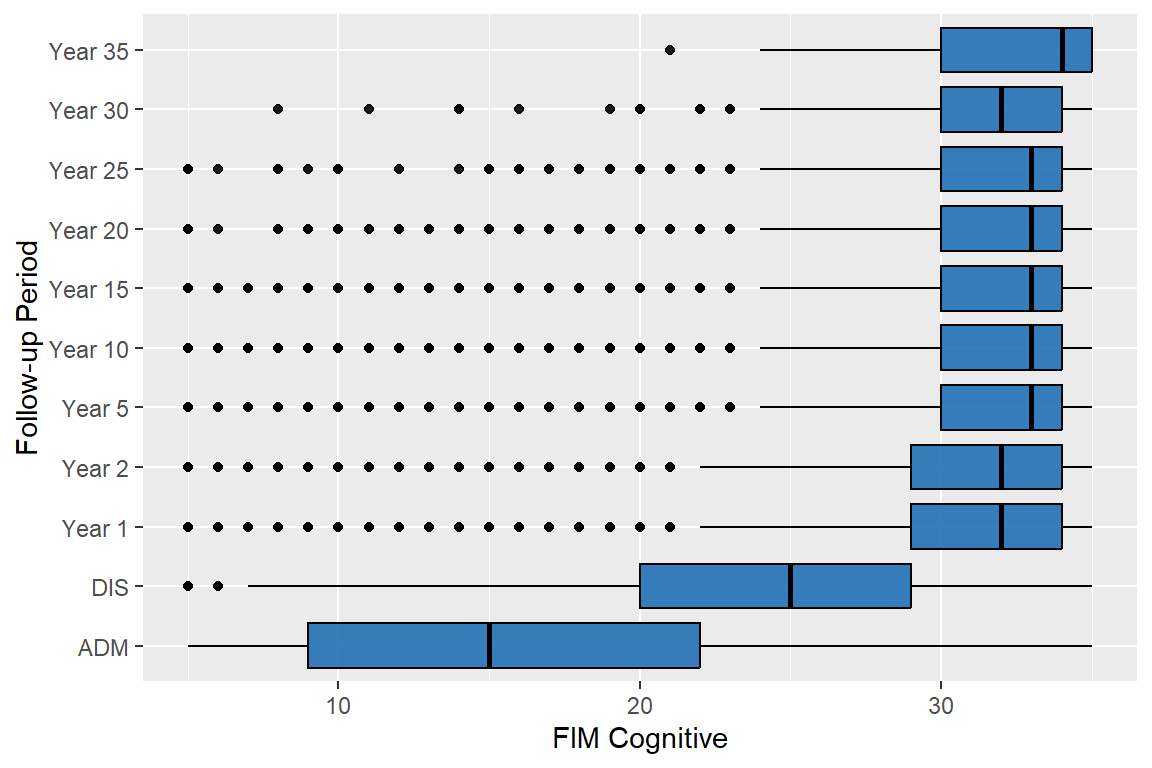
98% of the abstracted people have valid data
94% of the interviewed people have valid data
| FIM Motor | |||||||||||
| Characteristic | ADM N = 18,309 |
DIS N = 18,309 |
Year 1 N = 17,114 |
Year 2 N = 15,144 |
Year 5 N = 11,895 |
Year 10 N = 8,062 |
Year 15 N = 4,984 |
Year 20 N = 2,469 |
Year 25 N = 875 |
Year 30 N = 255 |
Year 35 N = 39 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| FIMMOT | |||||||||||
| N Non-missing | 17,454 | 17,574 | 16,144 | 14,212 | 11,193 | 7,505 | 4,597 | 2,261 | 749 | 217 | 30 |
| Mean (SD) | 36 (18) | 66 (19) | 82 (16) | 83 (15) | 84 (14) | 85 (13) | 85 (13) | 85 (13) | 85 (13) | 85 (11) | 82 (17) |
| Median (Q1, Q3) | 34 (19, 49) | 69 (57, 80) | 89 (82, 91) | 90 (84, 91) | 90 (85, 91) | 90 (86, 91) | 90 (86, 91) | 90 (86, 91) | 89 (84, 91) | 88 (83, 91) | 91 (82, 91) |
| Min, Max | 13, 91 | 13, 91 | 13, 91 | 13, 91 | 13, 91 | 13, 91 | 13, 91 | 13, 91 | 13, 91 | 19, 91 | 13, 91 |
| Missing | 855 | 735 | 970 | 932 | 702 | 557 | 387 | 208 | 126 | 38 | 9 |
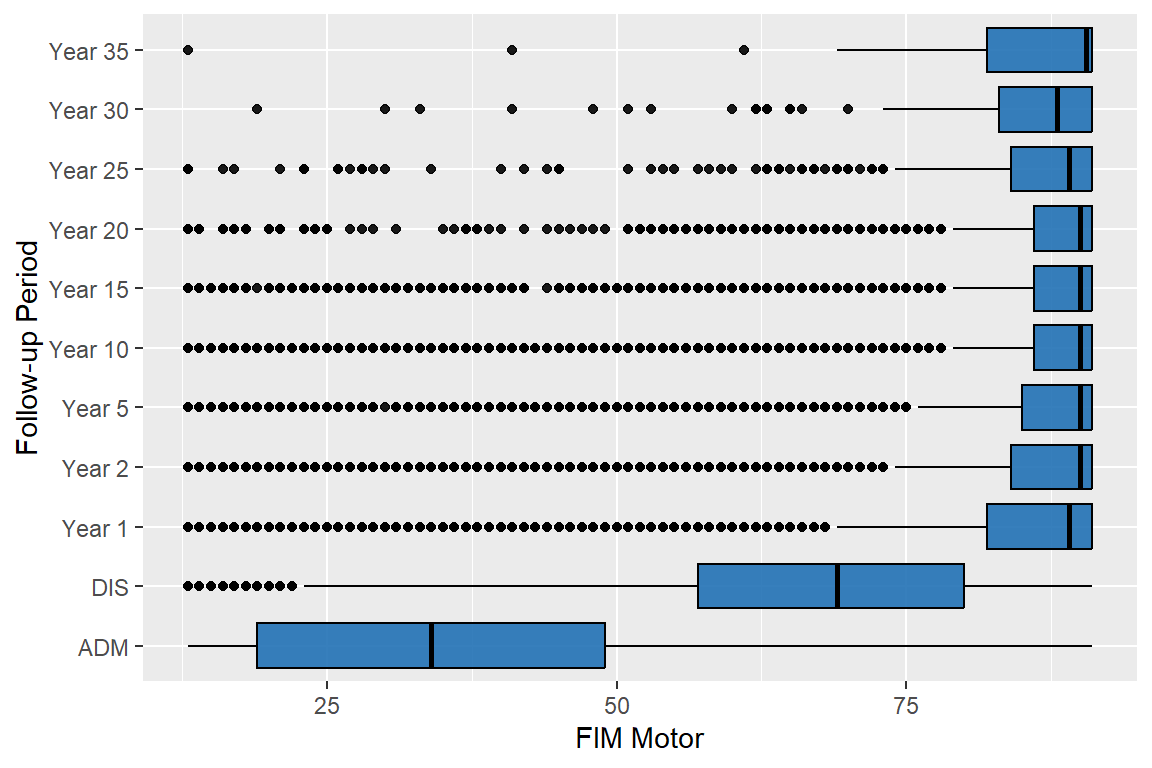
95% of the abstracted people have valid data
94% of the interviewed people have valid data
Date Added : 1989-10-01
DRSa refers to Disability Rating Scale at admission (collected at Form 1)
DRSd refers to Disability Rating Scale at discharge (collected at Form 1)
Disability Rating Scale ratings are to be completed within 3 calendar days for each assessment period. Indicate ratings for all items. Information about the DRS is available from COMBI. See External Links
The DRS at Form 2 (DRS PI) is a standardized questionnaire, and questions should be asked the same way every time with no words changed. If the participant is having trouble understanding the question, restate the question as phrased. If additional clarification is needed, then data collectors can rephrase the question or offer clarification.
[X] Form 1
[X] Form 2
Form 1 - To be completed by clinician or other individual who is trained and certified to code the DRS.
Form 2 - Interview (participant or proxy)
Form 1
If DRS assessments cannot be completed within the 3 calendar day window, they should still reflect the patients’ status within that time period. If this is not possible and the assessments are done out of the 3 calendar day window, code “Unknown”.
Every effort should be made to obtain the DRS assessments, however, if any items can not be assessed, use code “Unknown”. Do not leave blanks.
If a patient has an intermittent acute care stay during inpatient rehabilitation, use the DRS scores from the first rehabilitation admission and the last definitive discharge. In addition, if a patient has an intermittent stay which is longer than 30 days, it is then considered a system discharge and the discharge date from rehabilitation is the system discharge date and the DRS scores should correspond to that date.
Form 2
The DRS for Form II is a standardized questionnaire, and questions should be asked the same way every time with no words changed.
If the answers to specific questions are obvious from answers given prior to the DRS questions, they may be confirmed and skipped.
If the participant is having trouble understanding the question, restate the question as phrased. If additional clarification is needed, then data collectors can rephrase the question or offer clarification.
If in doubt on how to code a response to a DRS item, give the participant the benefit of the doubt. For example, if a participant states that they can give you the correct date and time, but is uncomfortable saying yes because it sometimes takes them up to 30 seconds, give them the credit for being able to do this.
Item Definitions (COMBI)
Properties (COMBI)
FAQ (COMBI)
DRS Training (COMBI)
DRS References (COMBI)
DRS Rating Form (COMBI)
DRS Introduction (COMBI)
PubMed:Rappaport M, et al (1987)
Rappaport M, Hall KM, Hopkins K, Belleza T, Cope N. (1982). Disability Rating Scale for severe head trauma patients: Coma to community. Arch Phys Med & Rehabil, 63:118-123. rev 8/87. For an abstract of this article, see External Links
Malec JF, Hammond FM, Giacino JT, Whyte J, Wright J. (2012) A Structured Interview to Improve the Reliability and Psychometric Integrity of the Disability Rating Scale. Arch Phys Med & Rehabil,Epub 2012 Sep;93(9):1603-8.
For follow-up, interviewers were originally rating the individual DRS items using the original DRS scoring form. The DRS structured interview was implemented on 10/01/2012.
The DRS-PI provides a structured interview for administration of the Disability Rating Scale (DRS) over the telephone. Except for cases with very severe limitations (eg, minimally conscious), the scoring algorithm for the DRS-PI results in a score that is comparable to the original DRS. However, there are differences between the original DRS and the DRS-PI for cases with very severe limitations. The Motor item of the DRS was not included in the DRS-PI because almost all cases interviewed in the development of the DRS-PI obtained a zero response on this item. In addition, the scoring of the Communication item was altered so that no score above 2 can be obtained. Scoring of the Communication item was altered in this way because very few scores above 2 were obtained in the development sample and collapsing all categories above 2 resulted in better fit of the Communication item with the Rasch model on which the DRS-PI was based. The Eye Opening item of the original DRS was not included in the DRS-PI interview and automatically scored as zero because eye opening should be present in all TBI cases who survive several months or more.
The Expanded DRS-PI adds additional items the DRS-PI and results in a score with a less skewed distribution than either the DRS-PI or the original DRS.
Original DRS. In order to obtain a score similar to the original DRS using the DRS-PI structured interview, an attempt can be made to administer the Motor item over the telephone. This item is only included in the Caregiver version since the Motor score will be zero if the person with TBI is able to respond to the interview questions. The Communication is the same as for the DRS-PI/ Expanded DRS-PI but is scored differently. Scoring algorithms for the DRS-PI, Expanded DRS-PI and Original DRS are at the end of this document.
The development of the DRS-PI and Expanded DRS-PI is described in: Malec JF, Hammond FM, Giacino JT, Whyte J, Wright J. A structured interview to improve the reliability and psychometric integrity of the Disability Rating Scale. Arch Phys Med Rehabil 2012;93:1603-8.
Testing and certification of data collectors of this variable is required. It is available from the COMBI website. See external links for training and testing materials.
| Disability Rating Scale | |||||||||||
| Characteristic | ADM N = 21,526 |
DIS N = 21,526 |
Year 1 N = 17,114 |
Year 2 N = 15,144 |
Year 5 N = 11,895 |
Year 10 N = 8,062 |
Year 15 N = 4,984 |
Year 20 N = 2,469 |
Year 25 N = 875 |
Year 30 N = 255 |
Year 35 N = 39 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Disability Rating Scale On Admission | |||||||||||
| N Non-missing | 21,151 | 21,187 | 15,892 | 13,984 | 10,919 | 7,245 | 4,389 | 2,167 | 742 | 210 | 29 |
| Mean (SD) | 11.4 (5.5) | 6.3 (3.9) | 3.0 (3.5) | 2.7 (3.4) | 2.6 (3.3) | 2.5 (3.1) | 2.6 (3.0) | 2.5 (2.8) | 2.6 (2.8) | 2.8 (2.6) | 2.3 (2.7) |
| Median (Q1, Q3) | 10.0 (7.0, 15.0) | 5.5 (4.0, 7.0) | 2.0 (0.0, 4.0) | 2.0 (0.0, 4.0) | 1.5 (0.0, 4.0) | 2.0 (0.0, 4.0) | 2.0 (0.0, 4.0) | 2.0 (0.0, 4.0) | 2.0 (0.0, 4.0) | 2.0 (1.0, 4.0) | 1.0 (0.0, 3.0) |
| Min, Max | 0.0, 30.0 | 0.0, 30.0 | 0.0, 28.0 | 0.0, 28.0 | 0.0, 29.0 | 0.0, 29.0 | 0.0, 26.0 | 0.0, 28.0 | 0.0, 19.0 | 0.0, 14.0 | 0.0, 9.0 |
| Missing | 375 | 339 | 1,222 | 1,160 | 976 | 817 | 595 | 302 | 133 | 45 | 10 |
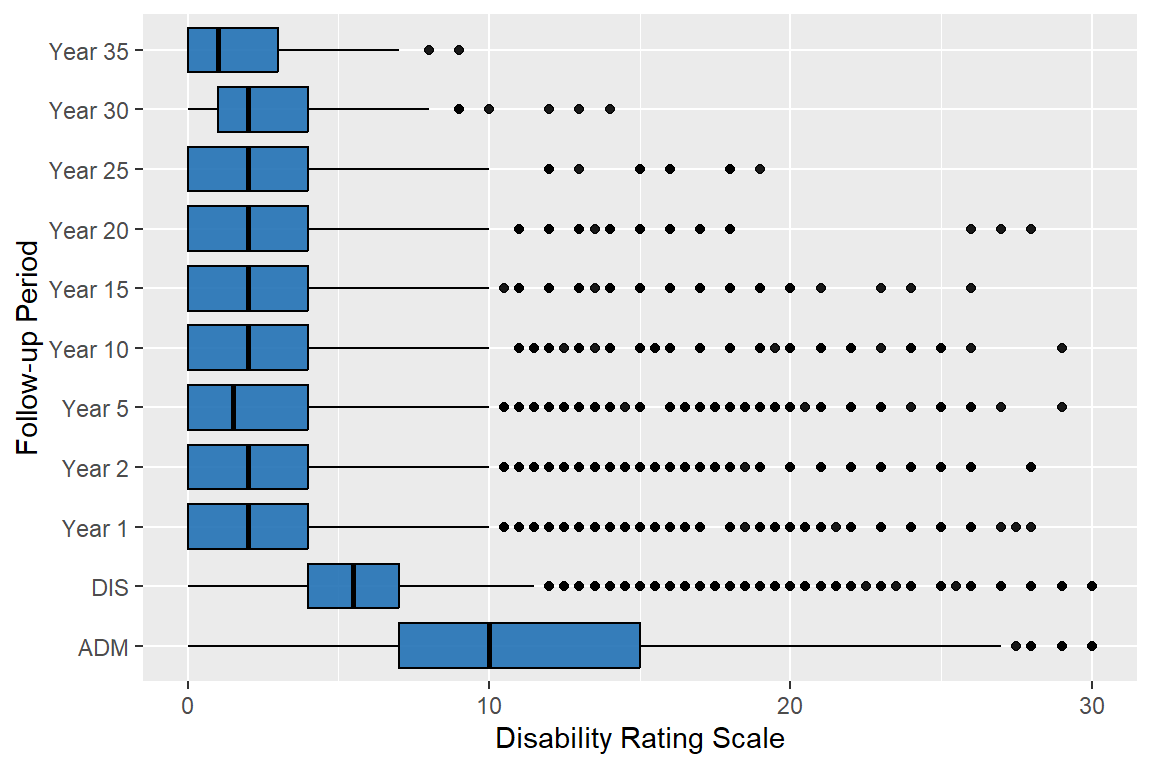
98% of the abstracted people have valid data
91% of the interviewed people have valid data
Date Added : 2020-07-01
The Continuity Assessment Record and Evaluation (CARE) Item Set was developed as part of the larger Post-Acute Care Payment Reform Demonstration (PAC-PRD), authorized by the Deficit Reduction Act of 2005. It was developed as a standardized set of items for measuring medical, functional, cognitive, and social support factors in the acute hospital, long-term care hospital (LTCH), inpatient rehabilitation facility (IRF), skilled nursing facility (SNF), and home health agency (HHA) settings to provide a way to compare the health status of Medicare beneficiaries across provider types.
Section GG Functional Abilities and Goals (Self-Care and Mobility Activities) includes admission and discharge self-care and mobility performance data elements. Qualified clinicians code each data element, which are activities, using a 6-level rating scale to reflect the patient’s/resident’s functional abilities based on the type and amount of assistance provided by a helper. If the patient/resident did not perform the activity and a helper did not perform the activity for the patient/resident during the assessment period, one of four “activity not attempted codes” is used.
The 6-Point Scale and Activity Not Attempted Codes
Coding:
Safety and Quality of Performance - If helper assistance is required because patient’s/resident’s performance is unsafe or of poor quality, score according to amount of assistance provided.
Activities may be completed with or without assistive devices.
01 - Dependent - Helper does ALL of the effort. Patient/resident does none of the effort to complete the activity.
Or, the assistance of 2 or more helpers is required for the patient/resident to complete the activity.
02 - Substantial/maximal assistance - Helper does MORE THAN HALF the effort. Helper lifts or holds trunk or limbs and provides more than half the effort.
03 - Partial/moderate assistance - Helper does LESS THAN HALF the effort. Helper lifts, holds or supports trunk or limbs, but provides less than half the effort.
04 - Supervision or touching assistance - Helper provides verbal cues and/or touching/steadying and/or contact guard assistance as patient/resident completes activity. Assistance may be provided throughout the activity or intermittently.
05 - Setup or clean-up assistance - Helper sets up or cleans up; patient/resident completes activity. Helper assists only prior to or following the activity.
06 - Independent – Patient/resident safely completes the activity by him/herself with no assistance from a helper.
If activity was not attempted, code reason:
77 - Patient/resident refused
81 - Not applicable - Not attempted and the patient/resident did not perform this activity prior to the current illness, exacerbation, or injury.
82 - Not attempted due to environmental limitations (e.g., lack of equipment, weather constraints)
83 - Not attempted due to medical condition or safety concerns
84 - Did Not Meet Criteria for Administration (To be used if participant leaves AMA, returns to ICU and does not return to rehab, or is only on rehab unit for 24 hours or less).
99 - Unknown No information, form not completed
[X] Form 1
[ ] Form 2
Abstracted from CARE tool data submitted to ERehab, UDS or CMS
Each core item for functional mobility is scored on a six-level rating scale measuring the need for assistance- dependent, substantial assistance, partial assistance, supervision or touching assistance, set-up or cleanup assistance, or independent.
Code “84 - Did not meet criteria for administration” to be used if participant leaves AMA, returns to ICU and does not return to rehab, or is only on rehab 24 hours.
Final IRF-PAI Version 3.0 - Effective October 1 2019 (FY2020) (PDF)
IRF-PAI Manual Chapter 2 - Section GG v3.0-508C
CARE Tool was added on 10/01/2019.
| CARE-SelfCare | ||
| Characteristic | ADM N = 3,217 |
DIS N = 3,217 |
|---|---|---|
| N Non-missing | 3,025 | 3,078 |
| Mean (SD) | 20 (8) | 32 (9) |
| Median (Q1, Q3) | 21 (14, 26) | 32 (27, 40) |
| Min, Max | 7, 42 | 7, 42 |
| Missing | 192 | 139 |
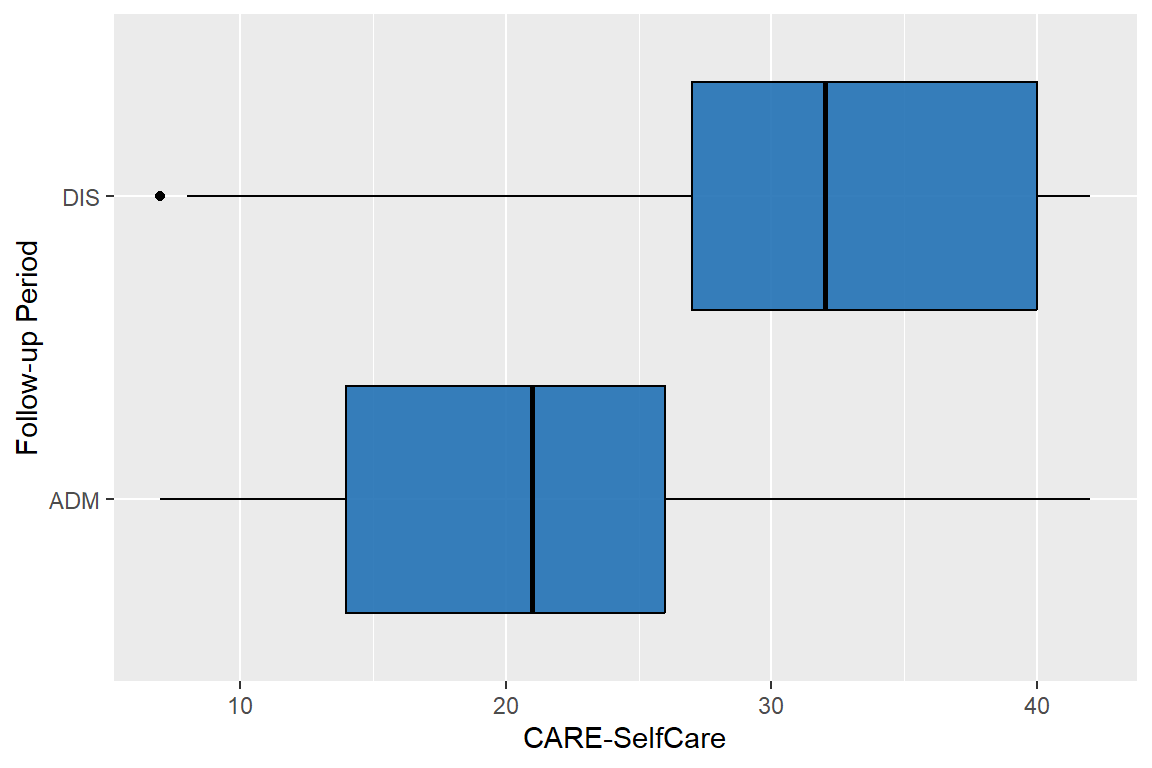
94% of the abstracted people have valid data
Date Added : 1998-04-01
For information about the GOS-E (Glasgow Outcome Scale-Extended), see External Links.
[ ] Form 1
[X] Form 2
Interview (participant or proxy)
Background of Instrument
The Glasgow Outcome Scale (GOS) was originally developed by Jennett and Bond as an examiner-rated measure of outcome. It has most typically been used to assess outcome in neurosurgery studies and has been widely used for clinical drug trials in acute TBI. The original GOS did not have a structured interview to accompany it. Raters, who may have been neurosurgeons, research nurses, or neuropsychologists, would give a GOS outcome rating based on all available information, including interviews with patients and their families, evaluation and examination of the patient, and any factual evidence they were able to obtain. Wilson et al. developed a structured interview to improve reliability of ratings on the GOS, as well as to extend the rating categories so that they would better characterize patients at different levels.
Instructions for Rating
The interview can be administered to either the patient or a family member or other informant. However, the GOS-E is not meant to be a self-perception instrument. Raters should rate each item based on the most accurate information they have, regardless of source. The following guidelines should help with the rating.
Although you are administering the interview to one person, you can obtain clarification from other sources if you feel that a particular item or items is inaccurate. For example, if the person with injury is the only person available to interview, you would administer the interview to him/her. However, if that person has limited insight into difficulties, and you know from another source that some of the answers are inaccurate, you can rate those particular items based on the most accurate information you have. For example, if someone who is in your post-acute program at the time of follow-up tells you they can travel without assistance, while their therapist says that they are medically restricted from driving and are currently receiving transportation training, you should assign the GOS-E score based on the information from the source that you feel to be most accurate. This does not mean that you are required to interview multiple sources. It just means that if you happen to have information from multiple sources, you can combine that information to increase the accuracy of your rating.
Many GOS-E questions overlap with other questions that you may have already asked as part of local or national database projects. It is not necessary to ask the question again for the GOS-E. If you already know the answer to a question, you can fill it in and move on to the next question. (Dr. Dikmen confirmed this with the authors of the GOS-E when we first began using it.)
Collect and record all subscale scores unless instructed to skip some of them by the skip instructions on the Form 2.
The intention of the GOS-E is to measure the person’s ABILITY to do things, whether or not they actually do them, so scoring should be based on what a person is able to do.
All raters should familiarize themselves with the original GOS-E article by Wilson and colleagues. Pay particular attention to the section on Assigning an Outcome Category (p. 576). This includes guidelines on how to account for pre-injury functioning.
Instructions for coding Unknown items
Every effort should be made to obtain the GOS-E assessment, however, if it can not be assessed, use code “99. Unknown.” Do not leave blanks.
There should not be many “unknown” answers from a respondent. If there are, then the respondent is probably not sufficiently informed about the person with TBI to be the basis for scoring the GOS-E. If there ARE many “unknown” responses and no better source of information is available, then the overall rating for the GOS-E should be “unknown”. Data collectors should use their judgment as to whether there are too many “unknown” responses to allow the GOS-E to accurately indicate the person’s level. Confer with your Model System’s data manager if uncertain.
For a GOS-E item that the respondent does not provide enough information to score other than “unknown”, the data collector should attempt to infer the score from alternative sources, such as the respondent’s answers to numerically higher GOS-E items, other items in the Form 2, and probes asked of the respondent and other persons informed about the person with TBI.
Additional Tips
Code deficits due to age as ‘Effects of Illness or Injury to Another Part of the Body’.
GOS-E is a “best source” variable. Not necessary to ask the two “supplemental” questions about seizures and source of disability (not present on data collection form).
The employment section can be based on education instead of employment if the participant was not working prior to injury. Evaluate whether the participant was attending school without difficulty (extra time, assistance, tutors, etc.). If the participant has returned to school part-time because she can not return to a full schedule due to the injury, then yes, code 5b as 1-Reduced work capacity. If you don’t have enough information to rate their schooling ability, you can skip the employment section and code as 88’s, and move onto the next GOS-E section.
If the person was unemployed and not seeking work before the injury, then they should be rated on the answers given to questions 6 and 7. For example, if the person is long-term unemployed or retired, then they should be rated on social and leisure activities and personal relationships. See external link, Wilson et al.- Frequently Asked Questions (p. 576).
The hierarchical nature of the GOS-E items causes lower items in the scale to not contribute to the overall score if the person is able to perform the task described by a higher item.
DATA ENTRY: Enter into the database all subscale scores that do not autofill. For each case that you enter, check to be sure that the auto-filled total score in the database is the same as the total score that has been recorded on the Form 2. Notify your Data Manager of any discrepancies.
DATA MANAGERS: If errors in calculating the total score turn up on the Form 2, provide your data collector(s) with more training in scoring the GOS-E and in calculating the total score. Contact the TBIMS NDSC if you have questions.
PubMed: JT Wilson, et. al. (1998) GOSE-Manual Frequently Asked Questions for GOS-E (COMBI) Properties of the GOS-E instrument (COMBI) GOS-E References (COMBI)
JT Wilson, L Pettigrew, G Teasdale. Structured Interviews for the Glasgow Outcome Scale and the Extended Glasgow Outcome Scale: Guidelines for their use. Journal of Neurotrauma, Vol. 15 No. 8, 1998. For an abstract of this article, see External Links.
For additional references, see External Links.
On 7/1/00 a field for data with the new scoring was created. The old field (data prior to 7/1/00) is also in the database. GOS-E data can be collapsed onto the GOS scale if analyses require.
| Glasgow Outcome Scale Extended | |||||||||
| Characteristic | Year 1 N = 17,317 |
Year 2 N = 15,235 |
Year 5 N = 12,742 |
Year 10 N = 9,231 |
Year 15 N = 5,633 |
Year 20 N = 2,802 |
Year 25 N = 1,018 |
Year 30 N = 298 |
Year 35 N = 51 |
|---|---|---|---|---|---|---|---|---|---|
| GOS-E Incl. Expired, n (%) | |||||||||
| 1 | 725 (4.5) | 498 (3.5) | 1,030 (8.6) | 1,169 (13) | 649 (12) | 333 (13) | 143 (16) | 43 (16) | 12 (27) |
| 2 | 85 (0.5) | 59 (0.4) | 46 (0.4) | 27 (0.3) | 14 (0.3) | 6 (0.2) | 3 (0.3) | 0 (0) | 0 (0) |
| 3 | 2,916 (18) | 2,216 (15) | 1,466 (12) | 879 (10) | 526 (10.0) | 238 (9.1) | 83 (9.1) | 36 (13) | 5 (11) |
| 4 | 2,212 (14) | 1,688 (12) | 1,058 (8.8) | 687 (7.9) | 414 (7.8) | 184 (7.0) | 74 (8.1) | 17 (6.3) | 2 (4.4) |
| 5 | 1,698 (10) | 1,637 (11) | 1,501 (12) | 1,194 (14) | 826 (16) | 454 (17) | 167 (18) | 53 (20) | 4 (8.9) |
| 6 | 3,182 (20) | 2,899 (20) | 2,405 (20) | 1,625 (19) | 986 (19) | 465 (18) | 153 (17) | 37 (14) | 6 (13) |
| 7 | 2,071 (13) | 1,930 (13) | 1,506 (13) | 1,040 (12) | 647 (12) | 304 (12) | 93 (10) | 20 (7.4) | 0 (0) |
| 8 | 3,334 (21) | 3,435 (24) | 3,022 (25) | 2,100 (24) | 1,213 (23) | 643 (24) | 200 (22) | 64 (24) | 16 (36) |
| Missing | 1,094 | 873 | 708 | 510 | 358 | 175 | 102 | 28 | 6 |
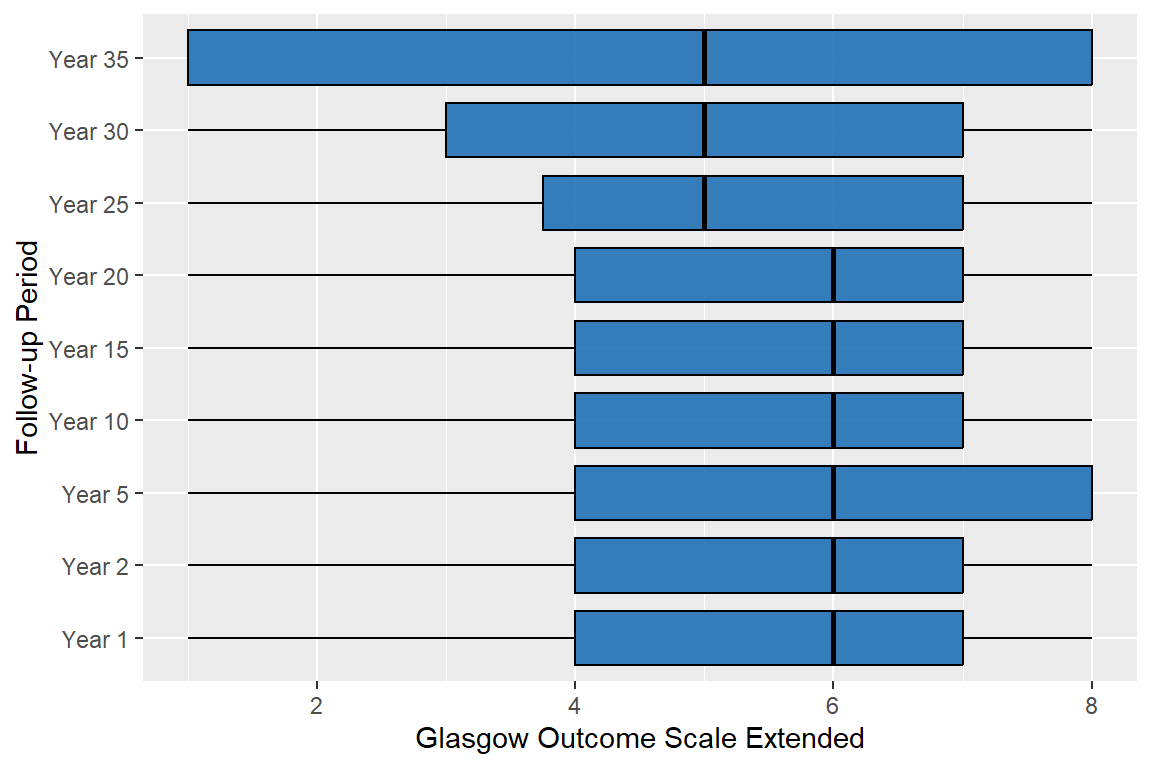
94% of the interviewed people have valid data